75 year old male with sob and b/l pedal edema
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome."
75 year old male k/c/o hypertension and diabetes presented to general medicine opd with the chief complaints of sob of grade 3-4
HOPI -patient was apparently asymptomatic 10 years ago when he was diagnosed with hypertension and diabetes mellitus ,for which he was prescribed medicine and patient used them religiously as he was working as a RMP himself , 2 years back patient developed b/l pedal edema and was taken to the hospital ,only to be diagnosed with chronic kidney failure and was prescribed medications which he used regularly but his pedal edema did not resolve ,patient has also undergone 2 sessions of dialysis last sesssion 18/10/2022 ,patient also complaints of several episodes of hypoglycaemia where in he’d sleep and on trying to wake him up he’d be unresponsive , everytime such an incident would occur he’d be visited by a doctor and would be given glucagon inj and was advised to take sugars such as Coca Cola or sugar while sensing such a feelings,also complaints of frequent episodes of fever for which he’d be given a paracetamol tab everytime
20 days back patient was laying down on his bed when he developed sob of grade 2 then progressed to grade 3-4 associated with b/l pedal edem and was immediately brought to Kims narketpally .
PAST HISTORY -patient is a known as of hypertension,diabetes mellitus since 10 years and ckd since 2 years .
DRUG HISTORY-Nicardia 20 mg ,Glimi-1 mg
FAMILY HISTORY - no significant family history
PERSONAL HISTORY- 75 years old married male with 5 daughter and one son ,worked as an rmp retired years back .
20 days back Patient was completely independent and would wake up at 6:00 am everyday and drink tea by 8:00 am while reading a newspaper and have adequate sleep and good appetite ,he’d take his medications by himself .
•Diet - mixed
•Appetite - reduced since 20 days
•Bowel and bladder - since the time being diagnosed with diabetes and hypertension patient complaints of increased micturation and defecation .
•Sleep - increased since 20 days and in a drowsy state .
•Addictions - patient used to consume alcohol and biddi 30 years down the lane
GENERAL EXAMINATION
patient is semiconscious, drowsy ,semi coherent and coperative
VITALS
BP-120 /70 mmhg
PR -88bpm, regular
RR-22cpm
TEMP -98 celcius
SpO2-92 percent at room air
Systemic examination
CVS
On palpation
Apex beat was felt in the 5 th inter coastal space medial to the mid clavicular line
Jvp was normal
No precordial bulge
No parasternal heave
-S1,S2 heard no murmurs
RS-
On inspection
Chest is b/l symmetrical
Expansion of chest equal on both sides
Position of trachea -central
No visible scars sinuses
On palpation
Expansion of chest was equal on both sides
Position of trachea -central
Tactile vocal fremitus -was felt
On percussion
all lung areas resonant
On auscultation
BAE + ,wheeze present
Vocal resonance - all areas resonant
PER ABDOMEN -soft no tender no organomegaly , bowel sounds heard
CNS -
All cranial nerves are intact functioning
Motor system examination
Normal bulk in upper and lower limbs
Normal time in upper and lower limb
Normal power in upper and lower limb
Gait is normal
Reflexes are normal
Sensory examination
Normal sensations are felt in all the dermatomes
NFND , HMF intact
No cerebellar signs
No meningeal signs
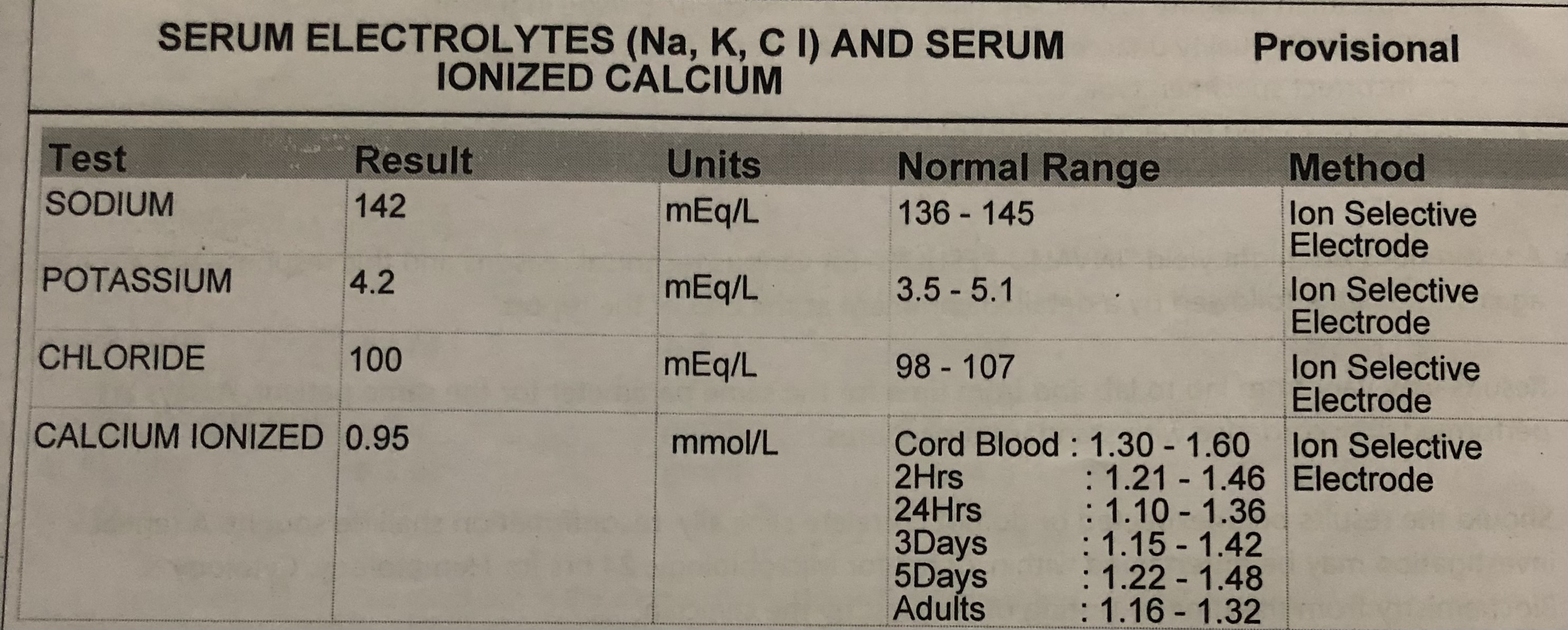
INVESTIGATIONS
RFT











Patient was also referred of ophthalmology consult to rule out hypertensive and diabetic retinopathy but was not found on complete examination
Patient was reffered for surgery consult in view of wound since 15 days
on examination
A 8x 6 cms lesions in anal region was found which was non tender no local rise of temp and sluff was present with dark pigmentation of skin ,no active discharge
A wound in the right hip region of 3x2 cms with pigmentation ,non tender ,no local ride of temp ,no active discharge .
A wound over right heel with dark pigmentation non tender no local rise of temp
Patient was advised regular change of position and movements along with regular dressings
PROVISIONAL DIAGNOSIS-CKD on MHD with diabetic neuropathy ?
K/c/o htn and type -2 diabetes mellitus.
TREATMENT
Tab.LASIX -40mg /po/BD
TAB.Met-XL -25 mg /po/OD
TAB.Nicardia -10mg/po/BD
TAB.Nodosis-500mg/BD
TAB.Orofer-XT po/BD
Inj EPO 4000U s/c weekly once
Salt water restriction
Inj HAI s/c acc to GRBS


Comments
Post a Comment